Showing posts from category Haiti.
-
Health Development: Providing Free Care and Overcoming Gender-Based Violence
›In The Lancet’s “How Did Sierra Leone Provide Free Health Care?,” author John Donnelly of the Ministerial Leadership Initiative attributes the unanticipated success of a free health care program for women and children in Sierra Leone to good organization, transparency, and a high degree of cooperation between the government, donors, and development partners. One distinctive factor that has contributed to the health system’s turnaround is the unusually high level of political will on the part of President Ernest Bai Koroma, writes Donnelly. Similar to Egypt’s health and population initiatives, Sierra Leone’s marked commitment, accountability, and investment as a host country has contributed highly to the success of its program and triggered further investment from donors. In “Systematic Violence: A Barrier to Achieving the Millennium Development Goals for Women,” from the Journal of Women’s Health, authors Joia S. Mukherjee, Donna J. Barry, Hind Satti, Maxi Raymonville, Sarah Marsh, and Mary Kay Smith-Fawzi assert that the elevation of women is integral to the achievement of the Millennium Development Goals, to which structural violence serves as a significant barrier. Murkherjee et al. recommend community-based programs to combat structural violence and prevent disease, such as the Partners in Health (PIH) program in Haiti. PIH trains community health workers, expands health care as a public good, and bolsters social determinants, which include increasing access to family planning and education, providing compensation for medical workers, and improving health infrastructure.
In “Systematic Violence: A Barrier to Achieving the Millennium Development Goals for Women,” from the Journal of Women’s Health, authors Joia S. Mukherjee, Donna J. Barry, Hind Satti, Maxi Raymonville, Sarah Marsh, and Mary Kay Smith-Fawzi assert that the elevation of women is integral to the achievement of the Millennium Development Goals, to which structural violence serves as a significant barrier. Murkherjee et al. recommend community-based programs to combat structural violence and prevent disease, such as the Partners in Health (PIH) program in Haiti. PIH trains community health workers, expands health care as a public good, and bolsters social determinants, which include increasing access to family planning and education, providing compensation for medical workers, and improving health infrastructure. -
Reporting on Global Health: A Conversation With the International Reporting Project Fellows
›“The story is the story, the information is the information, but you can frame it in very different ways,” said freelance journalist Annie Murphy at a roundtable discussion on the current state of global health reporting. Fresh off their five-week assignments, Murphy and three other fellows from the International Reporting Project (IRP) – Jenny Asarnow, Jill Braden Balderas, and Ann S. Kim – spoke at an event at the Woodrow Wilson Center on April 28 about their experiences researching underreported health issues in Haiti, Botswana, Mozambique, and Uganda. [Video Below]
Taking the Temperature of Global Health Reporting
Global health reporting, like many other forms of journalism, has felt the pinch from the global financial crisis, said Balderas, who edited a recent Kaiser Foundation report on the issue, “Taking the Temperature: The Future of Global Health Journalism.” Other challenges that have led to less global health coverage in mainstream media include an increased focus on “hyper-local” news; “story fatigue” from years of HIV/AIDS coverage; greater focus on epidemics and disasters; and the increasing number of advocacy groups starting their own news services.
Placing global health stories is a big challenge, agreed all four panelists. Who will want to run the story? What form – radio, documentary, print, online – will the story take? According to Murphy, some creative thinking may be needed: “It is global health, but that doesn’t mean we always have to frame it in this box of global health. It will be global health no matter what we do, so I think it’s also important for us to feed it into other events and issues that are important.”
(Re)building Maternal Healthcare in Haiti
With the worst maternal and infant mortality rates in the Western Hemisphere, Haiti needs medical providers of all kinds, said Asarnow, but especially skilled birth attendants. The devastating earthquake in 2010 destroyed Haiti’s only midwifery school, located in Port-au-Prince, killing many students and instructors. The school is still struggling to graduate a class of 15 people, she said.
In the rural town of Hinche, located in Haiti’s Central Plateau region, Asarnow frequently visited a public hospital that provided pregnant women with free obstetric care. Yet, she said, “even with free care, there [were] still a lot of barriers for women coming to the hospital to get care.” For example, the family members of expectant mothers had to provide sheets, clothing, food, and a bucket for personal needs. In addition, some women were too poor to afford transportation to and from the hospital.
Most women in Haiti, though, give birth at home with the help of traditional birth attendants, called matrones, Asarnow said. These matrones, popular in rural areas, are not formally educated in midwifery, but the government, along with non-profits such as Midwives for Haiti, have provided the matrones with training in basic health care and emergency situations.
Simply reporting on childbirth turned out to be a challenge, said Asarnow. “It’s hard to get people interested in something that just happens to most women,” she said; other more unusual health problems, such as infectious diseases, tend to garner more interest.
Finding Health Sovereignty in Mozambique
Health sovereignty, explained Murphy, is “the idea that nations have the right to make decisions about health and about how people are going to be treated” – an issue that is particularly pointed in Mozambique, where 50 percent of the national budget and 70 percent of the annual health budget is tied to international aid.
Mozambique, said Murphy, has only 1,000 doctors to serve a population of 22 million. By contrast, the country has an estimated 50,000 traditional healers. As a result, she said, most Mozambicans use traditional healing for at least part of their regular health care.
While researching traditional healers in the northern province of Tete, Murphy investigated a large Brazilian-owned coal mine that had displaced 5,000 local people when it was built. Mining is a major economic activity in Mozambique, yet mining companies are taxed a mere three percent by the government, said Murphy.
Health reporting doesn’t have to only cover traditional health issues, said Murphy. “The environment, natural resources, and how a country earns its money very much have to do with the health of the people who are living there,” she said. “How can you talk about being sovereign and providing health to your citizens if you don’t have the money to do that?”
Treating the Over-Treatment of Malaria in Uganda
“Malaria is quite over-treated” in Uganda, said Balderas. There’s the “idea that if you have a fever, you have malaria.” Consequently, the rate of misdiagnosis can reach alarming rates in some areas, she said.
Balderas said an estimated 50 percent of Ugandans get free treatment through the public sector. However, only donor-funded facilities are equipped with the rapid diagnosis test (or RDT), which takes only 20 minutes to determine the presence of malaria in a blood sample, she said. If these facilities were more widespread, misdiagnoses rates could easily be lowered.
Other challenges to the accurate diagnosis and treatment of malaria include faulty equipment, shortages of electricity and lab technicians, human error, corruption, bureaucratic entanglements, and presumptive diagnoses. For example, sometimes health workers do not know what is causing a patient’s fever, Balderas said, but they prescribe malaria treatments anyway because “they want to be able to give someone a treatment; they want to feel like they’re helping people.”
“There are certainly a ton of issues that relate to health,” Balderas said, such as poverty and corruption. Everyone she interviewed in Uganda – with the exception of government officials – identified the corruption in the country’s drug sector as a key problem.
Helping “Africa” One Small Story at a Time
Inspired by a World Health Organization study, which found “at least a 60 percent reduction in HIV infection among men who were circumcised,” Kim went to Botswana to investigate infant circumcision, a practice that is gaining popularity but is still alien. “I would meet people in the course of my day and they would ask me what I was doing there and I would talk about circumcision. They’d say, ‘Oh, I really want to get my baby circumcised. How do I do that?’” she reported.
The most powerful moment of her trip, said Kim, came when she was researching cervical cancer – the number one cancer among women in Botswana. As she waited with a woman to receive her lab results, Kim asked her if she was nervous. The woman, who was HIV-positive, said, “Yeah, I’m really worried. To me, it would be worse to get cervical cancer than to have HIV.” Even though Botswana is a middle-income country, said Kim, there are far more resources available to treat HIV than cancer.
Kim said that when presenting her work it was important for her to bring in the human element and not just the statistics: “I hope that, in whatever small way, even these small stories will help get issues in various countries on the map, especially in Africa where we tend to think of it as ‘Africa’ and not so much as different countries with different personalities and different situations.”
Sources: Malaria Journal, UNFPA, World Health Organization.
Image Credit: David Hawxhurst/Woodrow Wilson Center. -
The U.S. Government’s Response to Disasters: Myth, Mistakes, and Recovery
›“Major crises and disasters have massively changed over the last generation,” said Dr. Frederick Burkle, senior public policy scholar at the Woodrow Wilson Center and senior fellow and scientist at the Harvard Humanitarian Initiative. “We have to start a new narrative of what we need to do to address [them].”
To discuss the emerging and persistent challenges of disaster prevention, preparedness, response, and recovery, Burkle was joined by Paul Born, co-founder and director of the Tamarack Institute for Community Engagement; Leonard Doyle, Haiti country spokesperson at the International Organization for Migration; Arif Hasan, adviser at the Orangi Pilot Project and founder and chairman at the Urban Resource Centre; and Dr. Eliane Ubalijoro, adjunct professor at McGill University and member of the Presidential Advisory Council for Rwandan President Paul Kagame.
“Retrieving the Wisdom of Those in Need”
Unfortunately, disaster responses often fail to “listen and gain a corner on the obvious,” said Born, discussing the need for community engagement and healing in times of disaster and conflict.
After Hurricane Katrina, for example, the formal disaster response failed to use hundreds of available buses to evacuate people, leaving thousands of people stranded in the floods. “If people were engaged, had a role to play, knew what to do, were part of a team, would this have made a difference? Would those buses have been deployed to help people?” asked Born.
Effective disaster response must utilize “the assets, the skills, and the knowledge that are present,” concluded Born. For example, when the systems in place by the Philippine government in the village of Talba failed to give proper warning to evacuate from a volcanic eruption, “it was a parallel warning system, developed by the community, that warned people, on time, to vacate the area and avoid any loss of life,” said Born. Community preparedness and engagement led to better utilization of available humanitarian assets and mitigated what could have been a much more severe disaster.
The Changing Nature of Humanitarian Emergencies
Increasingly, humanitarian crises are the result of unconventional warfare, causing major challenges for the humanitarian community, said Burkle. Rather than refugees, “what we are beginning to see today is an unprecedented number of internally displaced people.”
Many of the displaced migrate to urban settings, contributing to rapid urbanization which is straining water, sanitation, and public health infrastructure. In these settings, he said, there is sometimes only one latrine for every 200 people, new and infectious diseases are rampant, and high rates of violence and rape are common, putting women particularly at risk.
“It is a lot more than population size – it’s really density of population,” said Burkle. In Mumbai, for example, there is an average of 30,000 people per square kilometer, but there are major areas of the city with over one million people per square kilometer.
“People moving to the cities are still remaining in extreme poverty,” said Burkle. While the majority of the poor once lived in low-income fragile states, recent population data indicates that 72 percent of the world’s poor now live in middle income countries like India, Indonesia, and China. “It’s a total reversal – we’ve spent almost 20 years crafting our foreign aid budgets and policy around this…we have to start a new narrative about what we are going to do.”
“The other issue that I don’t think we hear about, but certainly the young people in the audience will be dealing with on a daily basis, are the biodiversity crises,” said Burkle. “Of the 34 biodiverse areas, 23 have experienced prolonged conflict,” which has had major impacts on the availability of water, food, and energy in these regions, said Burkle.
Moving forward, “we have to change the humanitarian community; we have to have more accountability and more accreditation, leading to a blueprint for professionalizing the humanitarian field,” concluded Burkle.
Community and Communication in Haiti
A little over one year after the devastating earthquake in Haiti, 680,000 people remain internally displaced, said Doyle. “About half the population has moved out of the camps, and there is some congratulations to be given to the humanitarian community for organizing that,” he said. “But, when you look at the statistics…only a tiny fraction of these people have reached what you would call durable solutions such as sustainable housing.”
“There is clearly a problem… why has more progress not taken place given the number of international organizations there and the generosity of the funding?” asked Doyle.
“People have a right to communicate and there is a benefit in that communication,” said Doyle. To help make this possible in the Haitian displacement camps, he and his colleagues at the International Organization of Migration (IOM) set up 140 suggestion boxes. The response was amazing, he said, and with the help of a local Haitian organization, IOM has begun broadcasting some of the over 5,000 letters received on a daily radio show.
“We need to help create respectful conversations in countries where we do so much hard work but see so much of it go nowhere,” said Doyle. Information from the letters has been compiled into reports detailing the major challenges faced by people including a lack of jobs, education, and housing. These letters are being used as a monitoring and accountability mechanism through which Haitians can tell NGOs and donors the successes and failures of projects being implemented in their communities. “Through this communication you can see what the community needs, rather than what the experts tell you the community needs,” he said.
Engaging Local Communities
“Regions are sometimes so badly devastated [after a disaster], that to rehabilitate their agriculture, transport, water supply systems, is a very daunting task,” said Hasan. His home country of Pakistan faced all of these challenges after heavy rains and subsequent flooding wiped out 3,000 villages and affected over 20 million people last year.
“Without a governance system, you cannot provide rehabilitation or relief,” Hasan said, citing an added challenge for disaster response in many developing countries. Often the needs of the people are not translated in to policy actions, he said, and “there is a big difference between what people want and what politicians want.”
Hasan offered some insights on how the development community can work with local communities to improve disaster response, pointing out that “pre-disaster situations determine the effectiveness of relief and rehabilitation.” Existing mechanisms to provide development assistance can be used to efficiently deliver goods and services in emergencies, he said. By fostering “true partnerships” international NGOs can help communities and governments should manage reconstruction and relief efforts after disasters using local materials, labor, and technologies, he said. Engaging communities in reconstruction “can be a really important healing process.”
Recovery and Resilience
“When you have a community that has been reduced to ashes, how can you retrieve hope so that transformation can happen?” asked Ubalijoro, stressing the importance of building community resilience after disasters. “We’ve been talking about disasters, but it’s important to remember how we learn to dream again together.”
Baskets of Hope is a project that aims to help Rwandan women recover from the genocide by providing training and jobs weaving baskets that are sold internationally. In addition to providing a source of income, the project also provides information about health and nutrition. With this multi-pronged approach, Baskets of Hope helps families to recover and move forward. “There’s an interesting relationship between weaving these baskets that are allowing these women to have economic empowerment and what it requires after a time of trauma to reweave the fabric of society,” said Ubalijoro.
Youth who have survived man-made or natural disasters are particularly vulnerable, said Ubalijoro. She and her colleagues work to link Rwandan youth with Holocaust survivors so that they can share their memories, pictures, and stories with one another. “Retrieving the wisdom from those who have gone through the unimaginable and having them share their experiences shows youth that even though they’ve lost everything, there are ways to move forward.”
Sources: Conservation International, Institute of Development Studies, International Organization for Migration, USAID.
Photo Credit: “Pakistan Floods” courtesy of flickr user IRIN Photos. -
Watch: Frederick Burkle on Lessons from Haiti and Professionalizing Humanitarian Assistance
›April 20, 2011 // By Schuyler Null“Haiti – in terms of coordination – was a debacle,” said Frederick Burkle, senior fellow with the Harvard Humanitarian Initiative and a visiting scientist at the Harvard School of Public Health. Burkle, who is also a senior public policy scholar at the Wilson Center, said that after the 2010 earthquake, “the large majority of people who showed up were under the age of 30 and this was their first disaster event.”
As a result, “best practices did not necessarily occur,” Burkle said. “Ninety-five percent of the work is probably done by 45 of the major NGOs,” but, he said, the number of “mom-and-pop shows” and other small NGOs in “The Republic of NGOs” is in the thousands.
Non-healthcare providers ended up providing services that they were not trained to provide – even amputations, Burkle said. “We certainly relish the humanitarian spirit of those who show up, but we have to have some coordination to ensure that best practices occur and that it goes in the right direction.”
“The professionalization blueprint really calls for courses, curriculum, and best practice standards,” said Burkle. The Harvard Humanitarian Initiative is working with the UN Office for the Coordination of Humanitarian Affairs, World Health Organization, and others to provide these resources.
“There’s a movement afoot within the humanitarian community itself to finally professionalize the humanitarian profession,” Burkle said, spurred on, in part, by the poorly coordinated responses to events like the Haiti earthquake. -
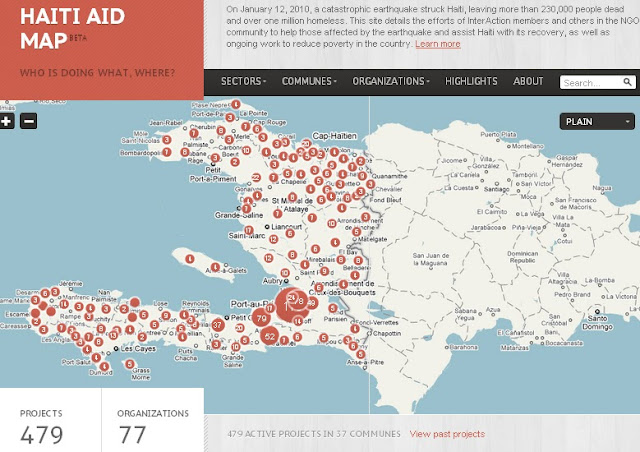
Mapping the “Republic of NGOs” in Haiti
›One year after the devastating earthquake that hit Haiti, InterAction has teamed up with the U.S. Chamber of Commerce’s Business Civic Leadership Center and FedEx to launch the Haiti Aid Map, an interactive visual mapping platform of individual aid projects being conducted in Haiti. The goals of the map are to increase aid transparency, facilitate partnerships, and help NGOs and others better coordinate and allocate resources to aid relief and reconstruction efforts.
With an estimated 10,000 NGOs operating on the ground – the second largest per capita in the world – Haiti has been referred to as “a republic of NGOs.” The Haiti Aid Map is an effort to help the humanitarian community – which has been criticized for lack of accountability, poor transparency, and corruption – better coordinate its response.
The map features 479 projects being operated all over the country by 77 local and international NGOs, most of which are InterAction members. Projects can be browsed by location, sector, or organization and include information on project donors, budgets, timelines, and the number of people reached by the project.While InterAction’s map covers their donors’ response, it leaves out the thousands of government and other NGO projects being conducted in Haiti. USAID recently released a map of U.S. government projects in Haiti (see right) by sector and location.
“The goal is not to rebuild Haiti but to build a different Haiti,” said Sam Worthington, President and CEO of InterAction, speaking exactly one year after the earthquake struck at the map’s formal launch this month. “The relief effort will still be here a year from now.” The goal of the map will be to help coordinate activities as reconstruction continues in the future.
The map is the first part of a larger mapping platform, called the NGO Aid Map, which will include not only the Haiti aid map but also projects working on food security in other developing countries. The food security map is due to be launched in March 2011.
Sources: Clinton Foundation, InterAction, NPR, ReliefWeb, USIP.
Image Credit: Adapted from Haiti Aid Map. -
Andrew Morton, UNEP
Haiti 2011: Looking One Year Back and Twenty Years Forward
›January 14, 2011 // By Wilson Center StaffThis piece first appeared on the website of the Haiti Regeneration Initiative – a new collaborative venture between the UN, the government of Haiti, the Earth Institute at Columbia University, Catholic Relief Services, and a wide range of other implementing partners.
In 2010, Haiti endured a year like no other. The country was struck by a devastating earthquake, a cholera epidemic, floods, violence, and political uncertainty. At the same time, Haiti witnessed heroic rescue and relief efforts and an enormous demonstration of international goodwill. Today, recovery and reconstruction are taking place, albeit at a frustratingly slow pace and not currently at the scale of existing needs.
Just as importantly, 2010 brought a renewed awareness of the need for lasting solutions and improvements in the design and delivery of international aid. During the next few days, we will look back on the tragic events of January 12th, 2010, while at the same time, we must look forward, not just one year, but 20.
A Failed Recovery in a Fragile State
Already before the earthquake, Haiti was a fragile state trapped in a slow but vicious negative spiral. A tightly interconnected trio of chronic environmental, political, and socio-economic crises has gradually ensured that Haiti has had the lowest human development indicators in the Western Hemisphere, with life-long poverty, chronic hunger, and violence. Catastrophic events, such as natural disasters, epidemics, and political violence, have simply steepened the descent. Moreover, disaster recovery efforts to date have systematically failed to bring the country back to pre-disaster levels.
In spite of this depressing analysis and forecast, we should not resign ourselves to failure. The situation can be turned around but only with great effort and by foregoing “business as usual.”
The first step towards change is full recognition of the situation. In the case of Haiti, this means recognizing the marked failure of foreign recovery and development assistance to date. It is pointless to blame any particular institution or individual for this: The current state of Haiti is the culmination of generations of efforts and decisions, good and bad, combined with rapid population growth and an inherent vulnerability to natural hazards. (Editor’s note: according to the UN, Haiti’s fertility rate tripled in the immediate aftermath of the earthquake last year.)
The second step is planning. While relatively solid recovery plans have been developed by the government of Haiti with international assistance, their implementation has not so far met with success, due to four interlinked problems.
First, the humanitarian imperative for urgent and chronic relief is overrunning all good intentions for recovery and development – it is politically impossible, inhumane, and simply unwise to ignore the basic resource needs of a cholera epidemic and a million people living in tents.
Second, nothing suppresses development investments like political violence and uncertainty: Few donors, and even fewer companies, will invest while riots and political uncertainty paralyze the country and destroy its reputation.
Third, the planning process is necessarily democratic and participatory; as a result, however, virtually all of the country’s needs are listed with no reliable process of thematic or geographic prioritization.
Finally – and perhaps most importantly – although the plans are official and uncontested, they generally lack broad credibility and commitment. Weary aid workers, government officials, donors and the general public look back at the fate of previous plans and, not surprisingly, expect these latest efforts to fail just as others have before.
Regenerating Haiti
Unlike virtually all other aid organizations I have met in Haiti, the team behind the Haiti Regeneration Initiative (HRI) has fortunately been given the vital time and seed funding to reflect on these issues and try something really different. After two years of preparation, on January 4, 2010, we launched a long-term rural sustainable development initiative for the southwestern tip of Haiti. The Côte Sud Initiative aims to transform the lives and the degraded environment of 200,000 people living in one of the poorest yet most beautiful parts of Haiti.
This specific initiative will only directly assist two percent of the population of Haiti, but just as importantly, we aim to demonstrate that sustainable development is truly possible in this country. Because national-scale issues require national-scale efforts, we also aim to promote change through dialogue and assisting the government of Haiti to develop and deliver on sustainable development plans that work. This is the primary mission of the HRI.
We must arrest the long-term decline as soon as possible. This includes, but is not limited to, basic recovery from the earthquake. At the same time, we need to establish the foundations for the long-term radical changes that are an absolute prerequisite to achieving sustainable development in Haiti. We must prepare to turn the vicious circles into virtuous ones.
So what are the short- to medium-term priorities?
The first is political stabilization, as vital foreign aid and direct foreign investment will simply not arrive in the face of such negative news and uncertainty.
Second, a massive aid investment in potable water and sanitation is required to suppress cholera in the longer term. No country can develop in the midst of recurrent major epidemics. This investment needs to be designed for sustainability; in other words, infrastructure needs to be accompanied by realistic, locally financed mechanisms for maintenance. Otherwise it will become useless within weeks of installation.
Third, persistence is needed on the current debris clearance and rebuilding efforts; we know from many other countries that such efforts can take years to be completed.
Finally, development aid should move out of Port-au-Prince and into the regions. In 2010, the massive influx of earthquake relief and reconstruction aid actually increased the economic pull of the capital and exacerbated existing urban problems.
What to do to prepare for the long term? Implementing radical change requires political support and even cultural reform, so in addition to good ideas, the HRI partnership will work hard to develop a sense of national ownership of the solutions as well as the problems.
Many of the ideas are not new: mildly decentralized development, diversified and value-added agriculture, niche tourism, improved aid coordination, public-private partnerships, etc.
Many, however, are radical, including a proposed paradigm change on migration and remittances, education, food security and import policies, widespread privatization, harsh revisions and rebuttals of traditional development models and assumptions, and adaptation to the new types of religious NGOs. These are just a few of the concepts and opportunities we have identified and will work to make a reality in Haiti.
Over the next few years, the HRI hopes to foster an intelligent and useful dialogue on sustainable development in Haiti. We look forward to having all of those who are concerned about and interested in helping Haiti join us in the debate.
Andrew Morton is the Haiti Regeneration coordinator and a senior staff member at UNEP. For more information on the Haiti Regeneration Initiative please see www.haitiregeneration.org.
Sources: BBC, Haiti Regeneration Initiative, United Nations Development Programme.
Image Credit: “Rebuilding as a community,” courtesy of flickr user Save the Children. -
The Cholera Quandary
›The original version of this article first appeared in the Stimson Center Spotlight series, November 19, 2010.
Cholera is usually seen as one of the most devastating infections of the 19th century. Trade routes carried cholera from India to the great cities of Europe and the United States. Disease, fear, and political unrest spread in great waves that cost millions of lives. After much destruction, it was only with science and resources that certain populations were able to curb the epidemic.One of the most celebrated lessons in the history of public health involves a cholera outbreak in London in 1854 and efforts by John Snow – celebrated as the father of epidemiology – to control it. At the time, it was not clear that cholera was a waterborne bacterial infection that caused severe diarrhea and vomiting, and sometimes fatal dehydration. Snow proved that the outbreaks decimating communities spread from contaminated water. Water and sanitation services had virtually eliminated cholera epidemics in the developed world by the early 1900s.
Today, cholera has been nearly eradicated in the developed world, but continues to be endemic in poorer countries. Risks seem to be rising as larger populations are crowded into unsanitary conditions. The World Health Organization (WHO) estimates three to five million illnesses and 100,000-200,000 deaths from cholera each year. If caught early, infections are treatable with inexpensive oral rehydration solutions. For much of the world, these options are unavailable or underused – the mere presence of cholera serves as an indicator of a country’s socioeconomic status and health system capabilities.
The cholera epidemics that are currently menacing countries on three different continents – Asia, Africa, and North America – raise tough questions about what is required to protect the world’s vulnerable populations. We know how to predict the crisis of cholera, prevent outbreaks, and contain them when they occur. To control cholera, what is needed is not cutting-edge technologies, but will, transparency, and resources – and where cholera appears, at least one of these three factors has failed.
Currently, cholera outbreaks in Pakistan, Haiti, and Nigeria are piling misery upon misery. Cholera in post-flood Pakistan comes as no surprise. When floodwaters left millions homeless and without access to clean drinking water in a region where cholera remains endemic, health officials could have reasonably assumed infected human waste would seep into water supplies and spread disease. The inability of health networks on the ground to prevent and then detect cholera demonstrates cracks in the country’s health system. What is apparent here is a lack of will and resources. Disease surveillance is especially vital in a post-disaster scenario where steps can be taken, such as treating water with chlorine, to prevent an outbreak.
Haiti had been free of cholera for at least 50 years, but the disease struck and spread rapidly 10 months after the devastating January 2010 earthquake. It reached Haiti’s capital and spread to its neighbor, the Dominican Republic. Since October, more than 114,000 people have become ill and more than 2,500 have died (Editor’s note: updated since original publication).
Haiti lacked resources for basic infrastructure even prior to the earthquake; the cholera crisis is not only costing lives, but also diverting aid from “building back better.” But regardless of the source of the cholera strain, if basic infrastructure and resources to protect Haiti’s vulnerable populations had been in place, cholera’s re-emergence would have been far less devastating.
This particular outbreak draws attention to the practical and political challenges of identifying health risks in humanitarian workers and peacekeepers, many of whom come from developing countries themselves. Evidence suggests that peacekeepers from Nepal, housed at a UN base, may have been the source of the outbreak clustered around the Artibonite River. Cholera outbreaks frequently exacerbate frictions between communities and aid workers – suspicions that have led to riots and murder more than once in recent years. At least two people were killed in Haiti in riots with peacekeepers during November.The delayed decision by the UN to investigate whether the outbreak originated with peacekeepers may have conserved resources for the race to stave off more cases, but did little to build trust between communities and foreign workers. Further violence and protests surrounding the recent disputed presidential election in Haiti do little to ease the devastation and in fact, threaten the relief effort. There has been discussion in Congress of cutting direct aid and suspending visas for Haitian officials until the dispute as been resolved. The Organization of American States is now reviewing the results.
In Africa, Nigeria is experiencing its worst cholera outbreak since 1991, and the disease is crossing borders. An onslaught of cases raised the 2010 death toll to more than 1,500 fatalities out of 40,000 cases. This mortality rate is three times higher than the seasonal cholera outbreaks of 2009, and seven times higher than 2008. Despite Nigeria’s oil wealth, most of the population is impoverished. Two-thirds of rural Nigerians lack access to safe drinking water and fewer than 40 percent of people in cholera-affected areas have access to toilet facilities, according to the Nigerian Health Ministry. A combined lack of will, transparency, and resources mean that cholera epidemics occur annually, and in clusters throughout sub-Saharan Africa.
A century and a half after John Snow’s discovery, we know how to control cholera. Globally, the resources exist, but the question of a collective will remains. For those who lack clean water to drink, to wash, or even proper toilets, the gap between knowing and doing is not easily closed. The international community has shown repeatedly that it can confront cholera outbreaks like those in Haiti, Pakistan, and Nigeria in the midst of crisis. The question remains as to how those efforts can eliminate the conditions that fostered outbreaks in the first place. The answer is not as riveting as the causes that often receive funding: basic infrastructure and resources. Roads, wells, clean water, toilets, education, and the willingness to recognize that if the foundation is not sound, nothing will be able to stand. Sometimes the simplest problems are the most difficult to solve.
Sarah Kornblet is a research fellow at the Global Health Security Program at the Stimson Center. Her research focuses on the International Health Regulations, health systems strengthening, global health diplomacy, the intersection of public health and security, and the potential for innovative and dynamic health policy solutions in developing countries.
Sources: Agence France-Presse, BBC, Washington Post, World Health Organization.
Photo Credit: “UN Peacekeepers Provide Security During Port-au-Prince Food Distribution,” courtesy of flickr user United Nations Photo. -
Judith Bruce on Empowering Adolescent Girls in Post-Earthquake Haiti
›“The most striking thing about post-conflict and post-disaster environments is that what lurks there is also this extraordinary opportunity,” said Judith Bruce, a senior associate and policy analyst with the Population Council’s Poverty, Gender, and Youth program. Bruce has spent time this year working with the Haiti Adolescent Girls Network (HAGN), a coalition of humanitarian groups conducting workshops focused on the educational, health, and security needs of the country’s vulnerable female youth population.
Gender-based violence has long been an issue in Haiti, but the problem became even more pronounced in the wake of the January earthquake. HAGN has sought to address the problem by concentrating its community-based programming on “high priority” groups, including girls who are disabled, serve as de facto heads of households, or are aged 10-14.
Bruce asserted that protecting and empowering young girls is critical because upon reaching puberty, “their access to a safe world shrinks dramatically.” With the post-disaster environment adding another layer of challenge, she said “there could be no ambiguity in anyone’s mind that we have to create dedicated spaces for girls who, at least for a few hours a week, feel secure to be themselves and to plan for their long-term safety as well as their development.”
The “Pop Audio” series is also available as podcasts on iTunes.