Showing posts from category Building Commitment to Family Planning.
-
Indonesia: Pioneering Community Outreach Creates Success Story
›January 31, 2012 // By Elizabeth Leahy MadsenThis is the third post in a series profiling the process of building political commitment in countries whose governments have made strong investments in family planning. Previous posts have profiled Rwanda and Iran.
While the two other countries profiled in this series, Rwanda and Iran, have only reinvigorated their family planning programs within the past 20 years, Indonesia’s story begins in the 1960s. In this respect, the world’s fourth most populous country is classified among the pioneers of family planning in the developing world and has been described as a “world leader” and “one of the developing world’s best.” An extensive community outreach program combined with a centralized government that made family planning a priority were key to Indonesia’s success story.
Jakarta Pilot and Religious Support Motivates National Scale-up
For a decade and a half after the struggle for independence from the Dutch ended in 1949, the government of President Sukarno ruled out any government support for family planning. According to a Demographic and Health Survey (DHS) report, the rate of contraceptive use among married women at the time was essentially zero. Fertility rose slightly during this period, from an average of 5.5 in the early 1950s to 5.6 children per woman a decade later. However, in 1965, Sukarno was overthrown, and the next year, a military general named Suharto assumed power in an uprising that left as many as half a million people dead.
Suharto’s regime would last until 1998. Though he operated with a “heavy hand” amidst personal corruption, Suharto also aggressively pursued economic development and brought about a policy shift towards promoting family planning. Despite initial reservations – Suharto believed that the people would oppose family planning on religious grounds – various domestic and international advisers convinced him otherwise.
General Ali Sadikin, the governor of Jakarta – a city of three million even then – was particularly influential in convincing Suharto. According to Australian demographer Terence H. Hull, who has written extensively about population issues in Indonesia, Sadikin was “quickly learning demographic lessons in his attempts to renovate a city with poor housing, schooling, transport, and basic services,” and he began to regularly speak out about the challenges that rapid population growth posed to his goals of urban development.Sadikin decided to support the Indonesian Planned Parenthood Association, which had a network of clinics offering family planning, but lacked the funding to meet more than a small amount of demand. With the public support of Sadikin, a Jakarta-wide pilot program was operational in 1967.
Hull reports that a second integral event in the early years was a 1967 meeting between government officials and Muslim, Protestant, Catholic, and Hindu leaders representing four of the country’s major religions. Following the meeting, a pamphlet called “Views of Religions on Family Planning” was published, representing “a tipping point when national consensus around the morality of birth control was turning from strongly negative to strongly positive.”
A Strong Coordinating Board Reaches out to Communities
By late 1968, efforts were in place to scale up the family planning program in Jakarta to the national level. The National Family Planning Coordinating Board (BKKBN in Indonesian) was created and quickly became entrenched throughout the country thanks to generous funding, including from international donors.
The BKKBN’s emphasis on the community level, which ensured that family planning services and awareness-generating activities were reaching people around the country through multiple channels, was a key factor in the program’s achievements. The organizations involved in promoting family planning messages at the community level included youth, women’s and religious groups, employers, and schools, with high-level support reiterated regularly by the president. Hull described the BKKBN’s efforts as “a true collaboration because the program emphasized institutions not normally associated with family planning, but did so in a way that was both socially acceptable and socially invigorating.”
In the program’s first two decades, the contraceptive prevalence rate for modern methods rose from almost nonexistent to 44 percent, and fertility subsequently fell from 5.5 to 3.3 children per woman. These changes are widely attributed to robust government sponsorship from the highest levels, together with effective grassroots implementation that fostered support from nearly all sectors of society.
In subsequent years, Indonesia experienced rapid economic and social development. Per capita income increased more than 20 times over between 1966 and 1996, with initial growth largely due to oil revenues. Other development indicators also improved dramatically. The literacy rate is now over 90 percent, nearly all girls attend school, and half of women are members of the labor force. However, Hull cautions against proclaiming the family planning program the primary causal factor in these successes. Family planning and other development programs would not have been as effective, he says, without changes in the political structure, which steadily became more centralized and stable in its oversight of a very heterogeneous society.
A Recent PlateauAs Indonesia continued to develop and its political system evolved, the family planning program has faced some challenges in the past 15 years. Suharto resigned in the face of widespread opposition in 1998, after more than 30 years in power. While this brought positive movement towards democracy, the ensuring political uncertainty shifted the government’s energies away from reproductive health and other aspects of social development.
In the early 2000s, the family planning program was decentralized to district and municipal levels, in line with political reforms aimed at diminishing the role of central hierarchy nationwide. District leaders were charged with planning, budgeting, and implementing family planning and other primary health services. In accordance, BKKBN modified its strategies to become even more community-oriented. Still, observers judge the family planning program to have “weakened” following decentralization.
With strong logistics, popular support, and donor assistance, contraceptive use continued rising during the years of political transition. By 2002-2003, 57 percent of married women were using a modern contraceptive method and the fertility rate had reached 2.6 children per woman. However, these indicators remained unchanged in the next national survey, conducted in 2007. Fertility in Indonesia is at the median for Southeast Asia – higher than Thailand and Vietnam and lower than Cambodia and the Philippines.
The Program Moves Forward
As democracy became more secure in the early 2000s, the country’s next generation of leaders kept sight of demographic issues. In 2005, President Susilo Bambang Yudhoyono stated, “High population growth without rapid economic growth will result in poverty and setbacks … Large numbers of children and high populations will only bring advantages if they are skilled.” BKKBN and the Ministry of Health worked with USAID, public health researchers, NGOs and others to develop national family planning standards for quality of care, which were devised and implemented in the early 2000s.
Judging the program’s achievements to have been substantial and its momentum sustainable, USAID graduated Indonesia from population assistance in 2006, after 35 years. Though gaps remain, women’s fertility preferences are largely being met.
Today, 80 percent of all births are intended, and unmet need for family planning – the share of married women who wish to delay or prevent pregnancy but are not using contraception – stands at nine percent, two percentage points below the average for Southeast Asia and all developing countries. Meanwhile, Indonesia’s demographic profile looks much different than it might have. At the time of graduation, USAID reported that without its long-standing and well administered family planning program, Indonesia’s 2006 population would have been larger by 80 million people, or 35 percent.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and senior technical advisor at Futures Group.
Sources: Demographic and Health Surveys; Hull (2007); Management Sciences for Health; New York Times; UN Population Division; USAID.
Photo Credit: “Jakarta,” courtesy of flickr user frostnova. -
Iran: A Seemingly Unlikely Setting for World’s Fastest Demographic Transition
›January 11, 2012 // By Elizabeth Leahy MadsenThis is the second post in a series profiling the process of building political commitment in countries whose governments have made strong investments in family planning. Read the first post, on Rwanda’s recent rapid demographic changes, here.
To date, only 11 countries outside of the developed world, China, and a handful of small island states have reached the end of the demographic transition, with fertility rates declining from more than four children per woman to replacement level or lower.* Of these, only two countries have completed the transition in 15 years or less – and both might surprise you. One is Cuba, whose government dispensed family planning services to its relatively small population in the 1970s through accessible primary health care facilities and legalized safe abortion eight years before the United States did. The other: Iran.
Following the 1979 revolution, Iran’s new theocracy adopted a socially conservative, pro-natalist outlook. Half of the population lived in rural areas, which typically constrains access to health services. In addition, abortion was illegal in most circumstances. According to the UN, Iranian women had an average of 6.5 children each in the early 1980s and the population was growing nearly four percent annually, a rate high enough for it to double in 19 years.
But, by the early 2000s, Iran’s fertility rate had dropped below two children per woman. The swift changes can be attributed to the efforts of government officials concerned about meeting the employment needs of a growing population, supported by public health experts who wanted to rebuild the eroded family planning program.
A Dramatic Policy ShiftThe turning point came after the end of Iran’s eight-year war with Iraq in 1988. With military demands high – several hundred thousand people were killed during the war – population growth was viewed positively. But as the war ended, policy directives did an about-face.
Although public health officials had framed the need for reinvigorated family planning programs in health-related terms for years, the motivation for government officials to change policy appears to have been economic. The national budget agency informed the prime minister that after nearly a decade of conflict, the country lacked adequate funding to both rebuild and to meet the needs of its people. The prime minister responded quickly, directing that demographic factors be integrated into the new development plan and stating that “Iranians’ standard of living was being eroded by the growth of the country’s population.”
“Pragmatism Has Prevailed Over Pure Ideology”
After convincing their superiors, Iranian government officials who supported family planning faced the added challenge of garnering the backing of the influential religious establishment. Shortly after the revolution, Ayatollah Khomeini officially sanctioned the use of contraception, though his perspective was not universal among clerics. Once the prime minister decided to introduce a national family planning program, officials sought support from additional religious authorities. Opposition was minimal after two key institutions offered endorsements. The High Judicial Council determined that there was “no Islamic barrier to family planning” in late 1988, and the Expediency Council approved the government’s plans soon after.
By late 1989, a new family planning program had been officially introduced. The program’s aims were to lengthen spacing between births; limit pregnancies in the early and late reproductive years; and lower fertility by educating the population and ensuring access to free and diverse contraceptive methods. By the mid-1990s, the government had fully integrated family planning into the existing primary health system.
Iran thus followed the example of other majority-Muslim countries where religion was not an impediment to family planning, including Egypt, Indonesia, Jordan, and Oman. Just as in countries where highly Catholic populations have low fertility rates (Italy, Poland, Spain, and many others), religious guidance has been interpreted in varying ways in different settings and is not necessarily a central factor in individual fertility decisions. As Akbar Aghajanian and Amir H. Merhyar write in a summary of Iran’s family planning program, “Pragmatism has prevailed over pure ideology when necessary.”
The Contributions of Women’s Education and a Strong Health System
A new policy orientation was the critical first step, but successful implementation was necessary for Iran’s demographic trajectory to change in response. Fortunately, the government had some advantages in rolling out its new program, namely a strong existing health system, a history of past efforts to promote family planning, and an educated female population among whom demand for contraception was high.Rural development became a priority of the government after the revolution and resulted in improved access to an array of services. In rural areas, community health workers receive two years of training to provide family planning services along with other preventative care and treatment. Services are also available at rural health “houses,” urban clinics, and higher-level centers around the country.
The status of women has also played a major role. A research exercise conducted by IIASA estimated that improvements in educational attainment among women were responsible for about one-third of Iran’s fertility decline between 1980 and 2005. Women’s literacy was already rising during the period of the revolution and reached 74 percent by 1996, while attitudes toward female employment became more supportive. By the late 1990s, new classes of university students included more women than men. The response to the 1989 program indicated that women clearly had an unmet demand for family planning. Use of modern contraception jumped from 31 percent in 1989 to 51 percent just five years later, then rose more slowly over the subsequent decade.
A Dividend Squandered?
The rapid changes in Iran’s age structure, thanks to declining fertility, have opened a window of opportunity for the country to boost economic growth through lower dependency ratios – a phenomenon called the demographic dividend. However, the dividend is not an automatic bonus, and Iran’s capacity to capitalize on its demographic change is questionable.
The unemployment rate among young people today is over 20 percent, indicating that the economy is not generating sufficient jobs, which is a prerequisite to improving productivity. This inopportune climate may even contribute to a further decline in the fertility rate: Some observers have suggested that the country’s economic troubles and rising costs of living have motivated young people to delay marriage and have smaller families. “Unemployment and high costs of living, coupled with social and political restrictions, have made [life] increasingly difficult for young Iranians,” Farzaneh Roudi of the Population Reference Bureau (PRB) explained in a blog post last year.
Given Iran’s challenges in producing adequate jobs and other economic benefits for its population, President Mahmoud Ahmadinejad’s recent unusual pronouncements on population issues are especially puzzling. Last year, Ahmadinejad introduced a pro-natalist policy offering direct payments to each child born, continuing until they reach adulthood, and later suggested that girls should marry at age 16 or 17.
But despite a high level of international media attention, most observers expect the policy to have little impact. Widespread adoption of family planning has become entrenched in society: 60 percent of Iranian women now use a modern contraceptive method. As PRB’s Roudi wrote in response to Ahmadinejad’s proposal, “Iranian women and men have gotten used to exercising their reproductive rights and would expect to be able to continue to do so.”
*The 11 countries that have achieved replacement fertility or lower outside of developed regions, China, and small island states are Brazil, Chile, Costa Rica, Cuba, Iran, Lebanon, Myanmar, Thailand, Tunisia, and the United Arab Emirates.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and senior technical advisor at Futures Group.
Look for related analysis on the political implications of Iran’s changing age structure by Richard Cincotta on New Security Beat soon.
Sources: Abbasi-Shavazi, Lutz, Hosseini-Chavoshi and Samir (2008), Abbasi-Shavazi (2002), Aghajanian and Merhyar (1999), Christian Science Monitor, GlobalSecurity.org, The New York Times, Noble and Potts (1996), Population Reference Bureau, Roudi-Fahimi (2002), UN Population Division, World Bank.
Image Credit: “بیست و پنجم خرداد ۸,” courtesy of flickr user Recovering Sick Soul (Nima Fatemi); charts arranged by Sean Peoples and Elizabeth Leahy Madsen. -
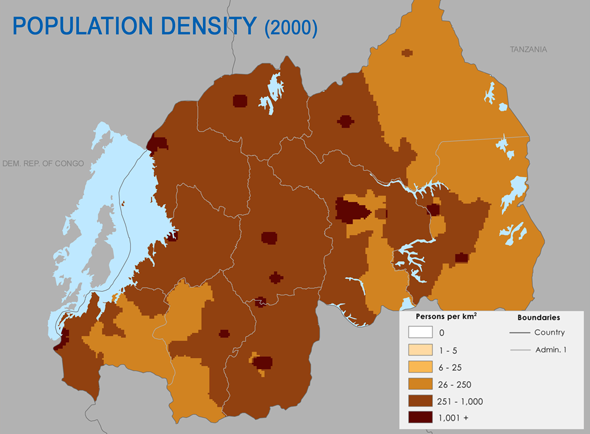
Rwanda: Dramatic Uptake in Contraceptive Use Spurs Unprecedented Fertility Decline
›November 8, 2011 // By Elizabeth Leahy MadsenWith over 400 people per square kilometer, the highest rate on the African mainland, population density is perhaps the most widely-discussed factor of Rwanda’s demography. Some scholars, notably Jared Diamond, have argued that it played a primary role in sparking the 1994 genocide through competition for land (although others present a more complex theory based in policies and governance).