-
Why Has the Demographic Transition Stalled in Sub-Saharan Africa?
August 7, 2013 By Elizabeth Leahy Madsen
In a recent post on the new United Nations population projections, I discussed the risk in assuming that countries in sub-Saharan Africa will progress through the demographic transition at a pace similar to other regions. Making this assumption is questionable because fertility decline in Africa has generally proceeded more slowly than in other parts of the world, with several cases of “stalls” and even small fertility increases over time.
While some countries have completed the transition from high to low fertility very quickly, others have stalled along the wayHowever, Africa’s demography is by no means uniform, and some countries and areas have developed distinctive fertility trends. At the regional level, the Southern African countries (Botswana, Lesotho, Namibia, South Africa, and Swaziland) had an estimated total fertility rate (TFR) of 2.6 children per woman in 2005-2010, about half the level of Eastern, Western, and Central Africa. Within those three high-fertility regions, the clear exception has been Rwanda, where a 25 percent fertility decline between 2005 and 2010 is the first of that speed and magnitude in sub-Saharan Africa.
What differentiates the countries in sub-Saharan Africa that are recording steady fertility declines from those where fertility has been stagnant or even rising? To explore this question further, I separated sub-Saharan African countries with multiple recent Demographic and Health Surveys (DHS) into two groups based on their fertility transition status.
Less Than Half of Sub-Saharan Africa Shows Significant Fertility Decline
Researchers have identified a decades-long process, called the “demographic transition,” during which populations move from high fertility and high mortality rates; to a period of low mortality rates and high fertility; and finally to both low fertility and low mortality rates, which creates the temporary opportunity for a “demographic dividend.” While some countries have completed the transition from high to low fertility very quickly, others have stalled along the way.
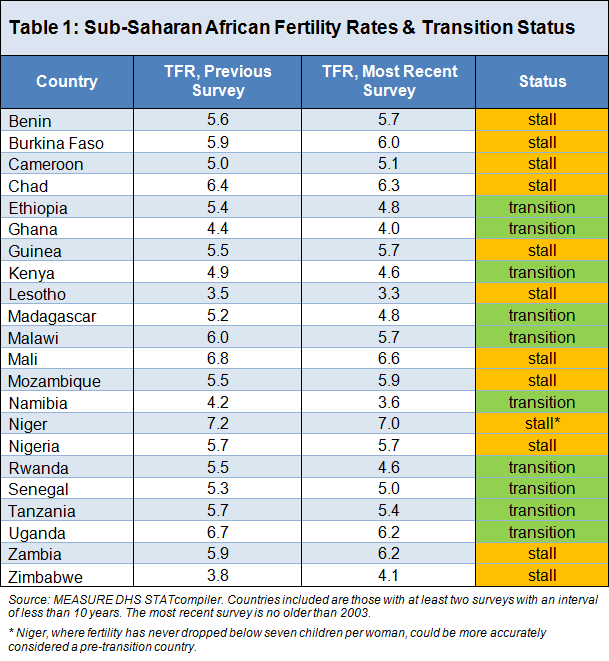
There are several possible methods of defining a fertility stall. A simple one is employed here: Sub-Saharan African countries were classified in the stalling group if the annual pace of fertility decline between their two most recent DHS reports was below 0.05 child per woman, about half the historical average rate of decline for developing countries in the late 20th century. This threshold represents a very slow rate of decline: The fertility rate in a country with an annual decline of 0.05 would take 20 years to drop by one child.

Of the 22 countries included in the analysis, 10 recorded an annual fertility decline of at least 0.05 child per woman between the two most recent surveys and are considered to comprise the group in transition. The remaining 12 countries are experiencing a fertility stall; half of them actually recorded a small increase.
As shown in Table 1, most of the countries with stalling fertility are located in West Africa. However, geography is not likely to be a cause of fertility patterns. What differentiates these countries in ways that may be relevant to their contrasting fertility transitions? The DHS provides rich data not only on fertility rates, but also on preferences and behaviors among women and men of childbearing age.
Stalling Countries Are High-Fertility Countries
The countries where TFR is stalling or increasing have a higher average fertility rate, at 5.6 children per woman, than the transition group, at 4.9. This may mean that fertility is more likely to be stagnant or fluctuating at higher levels and to then decline steadily once it has crossed below a certain threshold. Zimbabwe, which has the second-lowest TFR among all 22 countries but also experienced the most significant increase in fertility between its two most recent surveys, is a clear exception.
Only two-thirds of married women in Niger and Nigeria have knowledge of modern contraceptionKnowledge of at least one modern contraceptive method is nearly universal – above 90 percent in 18 of the 22 countries. A few countries in West Africa are outliers in this regard: Only two-thirds of married women in Niger and Nigeria have knowledge of modern contraception. In Chad, only 49 percent of married women have contraceptive knowledge, an extremely low level. Chad also has one of the lowest rates of modern contraceptive use in the world, at less than two percent.
The stalling countries share several characteristics of high-fertility countries compared to those in the transition group. Women in the middle of their reproductive years (ages 30 to 34) had their first child about six months earlier in the stalling countries, at age 19.5, compared to age 20 among the transition countries. Modern contraceptive use among married women is much lower among the stalling countries, with a median of 11 percent, compared to 28 percent among the transition countries.
Fertility preferences are important in shaping individual fertility behavior, and in most of sub-Saharan Africa, women and men prefer to have large families. Still, ideal family size is notably higher among the countries with fertility stalls, at an average of 6.0 children per woman, compared to 4.6 in the transition countries. In Chad and Niger, two of the stalling countries, married women report an ideal family size of nine children. Among the transition countries, ideal family sizes range from 3.6 children in Rwanda to 5.5 in Senegal.
Large Desired Family Sizes, But Also Opposition and Health Concerns
In the stalling countries, women are actually somewhat more likely to have fewer children than their stated ideal. In Cameroon, Chad, Niger, and Nigeria, actual TFR is at least one child per woman below the mean ideal number of children, indicating that on average, desire to use family planning to limit childbearing is probably weak, although there may be interest in birth spacing. In only one of the stalling countries (Zambia) are women having at least one child more, on average, than their ideal family size; this is the case in three of the transition countries (Malawi, Rwanda, and Uganda) and suggests likely demand for contraception in those places.
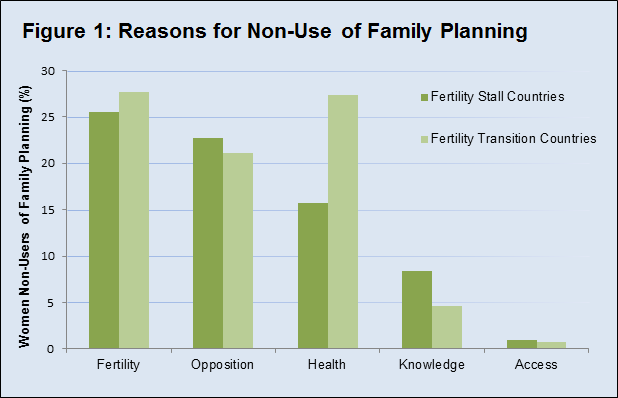
Previous models have shown that ideal family size and attitudes about family planning are important in countries’ national fertility transitions. The Demographic and Health Surveys ask women who are not contraceptive users to identify their main reason for non-use. Women’s responses can be grouped into five broad categories:
- Fertility-related: a woman believes that she cannot or will not get pregnant;
- Opposition: she, her partner, or religious beliefs oppose family planning;
- Knowledge: she does not know a method or how to obtain one;
- Access: she lacks physical or financial access to obtain a method;
- Health: she has health concerns about contraception or its side effects.
Although not a perfect measure, this information can help identify challenges that family planning programs face in expanding access to and use of services.
In the stalling countries, the percentage of women who say they are not using family planning because they want more children is about twice as high as in transition countries (22 to 12 percent). When these women are subtracted, the breakdown in reasons for non-use of family planning is fairly similar among the two groups. About one-quarter of non-users in all countries cite fertility-related reasons; that is, they are not using contraception because they believe they do not need to. Another one-fifth of women in all countries cite opposition, a taxing problem for family planning programs to overcome. In Nigeria and Senegal, opposition is the main reason provided by 40 percent of non-users.
The only reason for non-use of family planning that shows major differences between countries in fertility transition and those with stalling fertility is that of health concerns. Health-related reasons are offered by an average of 27 percent of women in transition countries, tied with fertility-related issues as the most common reason for non-use. In countries with fertility stalls, a relatively low 16 percent of women who are not contraceptive users cite health reasons.
Breaking From the Mold
In addition to the behaviors and preferences discussed here, many other factors could contribute to the variation in fertility transitions seen in sub-Saharan Africa. For example, the quality of national family planning programs in terms of funding, human resources, logistics, and political commitment, likely has significant influence. More broadly, demographers have found that increases in women’s education and improvements in infant and child mortality contribute to faster fertility declines. This is logical and highlights the contributions of multi-sectoral social development policies to demographic change. Education affects fertility through contraceptive use and age at marriage, and mortality decline precedes fertility decline in the demographic transition.
Not only are demographic transitions within Africa not following the mold of other regions, they are not following one anotherThe heterogeneity of African fertility transitions and their variance from historical patterns are important for planning and implementing family planning programs, but also have far-reaching development implications. The diverse reasons that women do not use contraception, as shown above, indicate an opportunity for governments and their partners to provide better information and education to potential users of family planning, to ensure that the quality of health services provided is high, and to improve the overall policy environment for health and for family planning in particular.
When making broader projections and plans that incorporate demography, it is critical to remember that previous expectations about what will happen in Africa may not hold, and fertility is unlikely to decline dramatically while desired family size remains high. The stalling fertility transitions across much of sub-Saharan Africa have motivated recent upward revisions in projections of the continent’s population, directly affecting the resources that will be required to improve economic well-being, human capital, and social resilience among a youthful, rapidly growing population. Not only are demographic transitions within Africa not following the mold of other regions, they are not following one another.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and senior technical advisor at Futures Group.
Sources: Bongaarts (2008, 1978), Ezeh et al. (2009), Kodzi et al. (2010), Lee (2003), MEASURE DHS, Shapiro and Gebreselassie (2008), UN Population Division.
Photo Credit: Market in Ibadan, Nigeria, courtesy of the International Institute of Tropical Agriculture. Chart and Table Credit: Elizabeth Leahy Madsen.
Topics: Africa, Cameroon, Chad, demography, development, family planning, featured, gender, Ghana, global health, Madagascar, Malawi, Mali, maternal health, Mozambique, Niger, Nigeria, population, Rwanda, Senegal, Tanzania, Uganda, UN, Zambia, Zimbabwe
 A Publication of the Stimson Center.
A Publication of the Stimson Center.