-
Rwanda: Dramatic Uptake in Contraceptive Use Spurs Unprecedented Fertility Decline
November 8, 2011 By Elizabeth Leahy Madsen
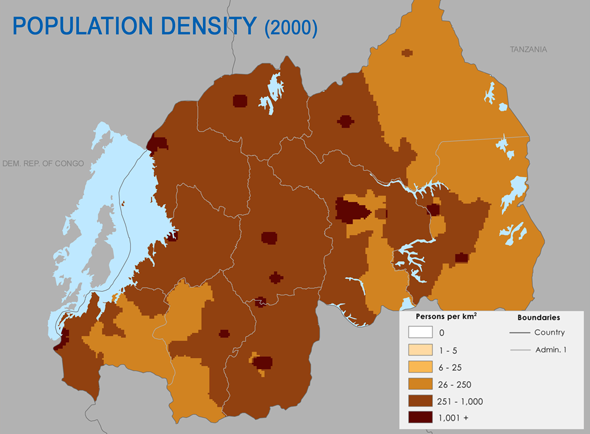
With over 400 people per square kilometer, the highest rate on the African mainland, population density is perhaps the most widely-discussed factor of Rwanda’s demography. Some scholars, notably Jared Diamond, have argued that it played a primary role in sparking the 1994 genocide through competition for land (although others present a more complex theory based in policies and governance).
Now, less than 20 years after the genocide, the country is experiencing demographic change of another sort, thanks to the government’s emerging reputation as one of the most committed to family planning on the African continent. Newly released preliminary data show a fertility decline that is unprecedented in its magnitude for sub-Saharan Africa. In 2010, Rwanda’s fertility rate was estimated at 4.6 children per woman, which represents a decline of 1.5 children per woman from the rate measured in 2005.
The Post-Conflict Years
In the early 1990s, Rwanda’s government stated support for family planning, publishing a National Population Policy that aimed to increase contraceptive use from two to 48 percent and consequently lower the average number of children born to each woman by more than half. However, fertility remained high (over six children per woman) and contraceptive use, low.
The 1994 genocide had a radical effect on Rwanda’s health system and skewed its demographic trajectory for several years. After nearly one million people were killed and even more displaced or fled, the population fell from 7.1 million in 1990 to 5.6 million in 1995.
This decline was short-lived. Use of modern contraceptives among married women fell from an already-low 13 percent before the genocide to just four percent by 2000. In addition to the practical challenges presented by a decimated health system and widespread poverty, traditional cultural and religious preferences for large families were accompanied by a strong desire to rebuild the population in the face of tragic losses. Rwanda’s population grew by 90 percent in 15 years, to 10.6 million in 2010.
Innovative Approaches Help Renew the Health Sector
 In the second half of the 1990s, efforts to rebuild health services after the devastating toll of the genocide began gradually, and family planning was not a primary focus. However, in response to declining use of health services following the introduction of user fees, the Ministry of Health in 2001 implemented a national network of mutuelles, innovative community-based health insurance schemes supported by member premiums and government funding. Over the past decade, mutuelles have been a major factor in improving Rwandans’ access to and use of health services, including family planning.
In the second half of the 1990s, efforts to rebuild health services after the devastating toll of the genocide began gradually, and family planning was not a primary focus. However, in response to declining use of health services following the introduction of user fees, the Ministry of Health in 2001 implemented a national network of mutuelles, innovative community-based health insurance schemes supported by member premiums and government funding. Over the past decade, mutuelles have been a major factor in improving Rwandans’ access to and use of health services, including family planning.In the 2000s, projects targeting the health sector were scaled up and international donors began implementing family planning projects, including service delivery and logistics and technical support. USAID’s contributions to family planning more than tripled, from less than $3 million in 2004 to $9 million in 2009. By 2005, increased demand for family planning was evident in the results of a Demographic and Health Survey. Although women were having an average of 6 children each, the reported desired family size was 4.3. Nearly 40 percent of married women did not wish to become pregnant but were not using contraception.
Government Commitment to Family Planning
In May 2005, the USAID-supported RAPID model, which was developed by Futures Group and quantifies the implications of family planning on other sectors, was presented to Rwandan parliamentarians, an event cited by many as pivotal in building support for family planning. The RAPID presentation served as a wake-up call, but with a positive message: besides making poverty reduction easier, having smaller families also increases health and education opportunities.
Parliamentarians were not the only political leaders who became interested in family planning. Ministry of Finance officials – whose influence over budgets is crucial in translating rhetoric to funding – also became convinced that high rates of population growth would inhibit their poverty reduction efforts. Rwanda’s current Economic Development and Poverty Reduction Strategy describes high population density as a pressure on the environment and on land use reforms.
The strategy establishes a target of reducing total fertility rate to 4.5 children per woman by 2012 (which preliminary survey results for 2010 indicate has nearly been achieved). The strategy also sets a bold goal to increase the rate of use of modern contraceptives to 70 percent among women of reproductive age. In addition, the strategy focuses on raising the proportion of the population with access to health centers and to improving the breadth of health care services offered at such facilities.
Dramatic Demographic Changes
In the past five years, concerted efforts have met much of this need, and are reflected in remarkable changes in demographic and reproductive health indicators. The five-year fertility decline of 25 percent is noteworthy for being the first decline of such magnitude in the region. (Similar fertility declines of 25 to 30 percent over five-year periods have occurred elsewhere since 1980 – Algeria, Cuba, Iran, the Maldives, Mauritius, Mongolia, Spain, and parts of East Asia, Eastern Europe and the Persian Gulf – but never in sub-Saharan Africa.)
Even more striking is the rapid increase in the share of married/partnered women using modern contraception, from 10 percent in 2005 to 45 percent in 2010. Improvements in the country’s health system are also reflected in other indicators: The share of mothers delivering in health facilities has increased from 45 percent in 2007-08 to 69 percent in 2010, and mortality rates have correspondingly improved. Infant mortality has fallen from 86 to 50 deaths per 1,000 live births, and the maternal mortality rate dropped by half between 2000 and 2008.
Rwanda’s centralized political hierarchy has been described as a key factor in the transmission of pro-family planning policies. As the most detailed study of political support for family planning in Rwanda has explained, “The government recognized the need to address population issues, so the policies were not imposed from the outside but were embraced and supported internally.”
The continuity of political support for family planning extends all the way to President Paul Kagame. After declaring the issue “priority number one” in 2007, he told an interviewer, “We recognize we are late on this.” Reflecting on the goal of increasing contraceptive prevalence from 10 to 70 percent in just four years, which many observers might judge unrealistic, a UN official observed, “Here you don’t say never when there is government commitment.”
An Emerging Success Story, But Not Yet Complete
While the recent trends indicating improved access to and utilization of health services are a major triumph for Rwanda, development challenges remain for the densely populated, agriculture-dependent economy. Only 21 percent of men and 16 percent of women have attended school beyond the primary level. And although Rwanda has made concerted efforts to rebuild social cohesion since the genocide, it remains at the center of a region where simmering conflicts flare up regularly across borders. Former perpetrators of Rwanda’s genocide continue to drive conflict and attack civilian populations in the eastern Democratic Republic of the Congo. In addition, international observers are raising increased concerns about authoritarian tendencies and limits on political opposition within Rwanda’s government.
Within the health sector, staffing levels have reportedly been low, and though progress so far has been remarkable, government funding for contraceptives must grow dramatically to meet rising demand. Despite the recent rapid decline in fertility rates and increased use of family planning, Rwanda remains a high-fertility country, and demographic momentum will drive continued population growth. Even if average family size falls below four children per woman, the population is projected to nearly double over the next 25 years.
Rwanda’s government has shown extraordinary interest in demographic issues and health system improvements, but as this is sustained, it must be matched with provision of education and jobs for the still-growing youthful population.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and senior technical advisor at Futures Group. She was previously a senior research associate at Population Action International.
Sources: Boudreaux (2009), Brookings Institution, Freedom House, Health Policy Initiative, Hewlett Foundation, MEASURE DHS, National Geographic, The New York Times, Pulitzer Center on Crisis Reporting, Rwanda Ministry of Finance and Economic Planning, Solo (2008), UN Population Division, USAID, Washington Post, World Health Organization.
Image Credit: Adapted from “Rwanda: Population Density, 2000,” courtesy of flickr user SEDACMaps; chart by Elizabeth Leahy Madsen.
 A Publication of the Stimson Center.
A Publication of the Stimson Center.